
How the GP crisis happened – and why it will get much worse.

For most of the last 25 years, there has been a war of attrition against Medicare. Nowhere are the effects more crippling than in general practice.
Fewer and fewer patients are being bulk-billed. Out-of-pocket costs are soaring. Medical graduates are shunning general practice for other higher-status, higher-paid specialties. Over vast areas of Australia, overworked practices are accepting no new patients at all. And research shows that major cities are about to experience the doctor shortages already entrenched in the regions.
HOW DID IT COME TO THIS?
There’s a history to it. Conservative parties fought against universal health care at every stage of its implementation. In the 1940s, the Curtin and Chifley governments’ attempts to create a national health scheme – but the Liberal and Country parties blocked it.
In 1974, the Whitlam government – after a double-dissolution election on the issue – finally established Medibank. But Malcolm Fraser, having promised before the 1975 election to maintain the program, dismembered and then privatised it.
The opposition to “socialised medicine” continued after the Hawke government was elected, but the numbers – and the popularity of the scheme – prevailed at last. In February 1984, Medicare became law.
In his push to win the 1996 election, when John Howard at last understood that opposition to Medicare was a vote-loser, he made no effort to disguise his lasting antipathy. “It’s not a question of whether it’s become better,” he said. “It is a question of us believing that Medicare is seen by the overwhelming majority of the Australian community as an important part of the social security infrastructure.”
So open warfare became a war of stealth and attrition. Private health insurance was heavily subsidised. Failure to invest in public hospital infrastructure increasingly compromised patient care.
The Howard government introduced a requirement for GPs to undergo an extra five-years of low-paid training, just like all the other specialties. But the government refused to pay doctors any more for all that extra training.
Rebates were subject to an indexation that failed to keep up with practice costs. When this became a political issue an inefficient and inadequate safety-net scheme was invented. Finally, rebates were frozen for over five years while practice costs continued to soar.
SO HERE WE ARE
The crisis hit the regions first and hardest. Figures from the Department of Health and Aged Care, the supply of GPs reveals two unequal Australias: in the major cities and large regional towns, you sill have a fighting chance of seeing a doctor. Further out, best of luck. You’ll need it.

The increasing difficulty of getting a GP consultation is shown in the data for waiting times, drawn from a national GP booking agency. They’re blowing out almost everywhere:

The RACGP and the AMA have often claimed that patients unable to see a GP are “flooding” public hospital emergency departments with low-urgency cases. It’s not true. It’s worse than that.
Until the pandemic lockdowns upended everything, non-urgent presentations at the nation’s EDs were in swift and substantial decline. People needing GP-type care knew they would be likely to wait for many hours to be seen and, according to ED staff, did not want to add to the already-crippling pressures in those departments.
So they stayed away. It’s increasingly the case that would-be patients unable to see a GP don’t see anyone else either. They remain untreated.

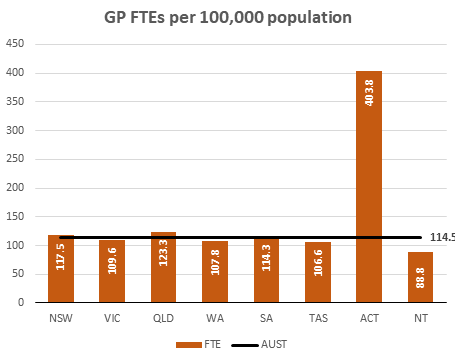
Supply – and shortages – are distributed fairly evenly across the states. The two territories are the exception, reflecting both income and urbanisation. The Northern Territory has only 77% of the national average of GPs per capita and 22% of the level enjoyed by the ACT.
It’s not that Australia doesn’t have enough doctors. It’s
that not enough of them are in general practice. Compared with OECD with which
we tend to compare ourselves, the number of practicing doctors per 1,000
population is well above the average.

Of these nations, only Germany and Sweden have more.

Nor is it true that we need to train more medical students. The OECD figures suggest the opposite: that we’re actually training too many.


The Royal Australian College of General Practitioners, which oversees GP training and standards, has reported a decline of 30% in medical graduates applying for GP training in just five years since 2017. “We are at serious risk of running out of GPs,” said Dr Karen Price, the college’s president.
STARVING MEDICARE
After a quarter-century of parsimony, Medicare funding has fallen far behind the real costs of providing care. When Medibank was introduced in 1974, it set the cost of a standard GP consultation at $8.20. In today’s CPI-adjusted dollars, that’s $70.71. But today’s Medicare rebate is just $39.75. That’s a shortfall of $30.96, or 43.8%.
Although the federal government requires general practitioners to have the same level of training as other specialists, GPs are paid much less. A survey by Alecto Australia, a medical recruitment firm, showed a full-time GP in a bulk-billing practice earns on average $253,000 a year; for the 25% working part-time, it was $194,000.
Specialists, particularly in private practice, can earn a great deal more. Another recent survey showed that neurosurgeons were the top-earning profession in Australia, with an annual average of $600,387. Ophthalmologists came second, on $533,511; plastic and reconstructive surgeons were third, on $500,269. But these are taxable incomes – what’s left after deductions and tax-minimisation techniques such as family trusts.
But senior practitioners can earn much more. Specialists in private practice work either in their own consulting rooms or in private hospitals. They bill patients directly, who have no effective pricing power. Practitioners at the peak of their professions – particularly senior surgeons and anaesthetists – can earn as much as several million dollars a year.
Inevitably, general practitioners – who work just as hard, have at least as much responsibility and have completed equal levels of training – ask why they are valued so much less.
So while GPs want status and incomes closer to those of other specialists, the money coming from Medicare has strikingly declined. Doctors protect their incomes by charging patients rather than the government: billing declines, out-of-pocket costs rise, and more people are shut out of medical care.
Data from the Australian Bureau of Statistics show that in an average year, more than 600,000 people delay or avoid going to a GP because of cost. And more than 900,000 delay or avoid filling a prescription because they can’t afford it.
The official Medicare statistics reveal the increasing amount paid by patients who are not bulk-billed:

BULK-BILLING FIGURES ARE A SCAM
Greg Hunt, health minister in the Morrison government, was fond of proclaiming record-high rates of bulk billing in general practice.
Superficially, they look very good. For a long time, most people believed them – even though there was a serious inconsistency between these figures and people’s experience in trying to find a bulk-billing doctor.

The figures are, of course, misleading. They refer to GP services, not just consultations. If, for instance, a doctor may bulk-bill for removing a wart, but charge a substantial co-payment for the consultation itself. The RACGP’s calculations show this factor alone should reduce the proportion of bulk-billed consultations to below 69%.
But that’s not all. Quirks in the billing process reduce the real figure even further. Dr Margaret Faux, a Medicare administrator, wrote a PhD thesis on these issues.
Some practices bulk bill, but put through gap charges as separate Eftpos transactions. That shows up in the statistics as a bulk-billed item. Others are plain dishonest in their billing practices.
 |
| Faux ... dodgy billing |
“The most common type of fraud in Australia occurs when a doctor knowingly bulk bills for a service they didn’t provide. It is devilishly difficult to find and therefore prosecute.
“There is also what I would describe as ethically questionable billing, caused by system dysfunction. The most common example is repeatedly returning patients for additional appointments, with the sole purpose of enabling more bulk billing.
“When I explained to a patient that his GP had spent more than 20 minutes undertaking complex work, he was horrified … the GP had apparently taken less than five minutes to write a prescription and order a blood test.”
The whole Medicare system, Dr Faux believes, has become so impossibly complex and opaque that “effective oversight by the Australian National Audit Office may no longer be possible for the simple reason that you cannot audit what you cannot see.”
In her 2021 thesis, she estimated that non-compliant billing – some deliberate, some not – cost Medicare between 5% and 15% of its total cost: that is, somewhere between $1.2 billion and $3.6 billion every year. General practice accounts for 32% of all Medicare benefits, so if the problems were spread evenly across specialties, the GP-specific cost to the system would be between $380 million and $1.7 billion.
There is another side to this argument. Many practice owners say their businesses are on the edge of financial failure, caught between the salary demands of their GPs, inadequate funding from Medicare and an unwillingness to put too much pain onto patients. In those cases, bending the rules may be the most ethically responsible thing to do.
AND NOW WHAT?
Australia actually has a National Medical Workforce Strategy. The document was released by the Morrison government in March, just two months before it lost office at the federal election, and claims to be a blueprint for action for the next decade. But nowhere in its 98 pages does the strategy analyse where the future shortages will occur or what will drive them. Its recommendations consist solely of small-scale tinkering within the existing system. On the central question of the adequacy of Medicare funding, it is silent.
Australia once had the capacity for making these forecasts but lost it when Tony Abbott defunded Health Workforce Australia in 2014.
So we must turn to the scattered analyses commissioned by commercial firms. The most significant of these was conducted by Deloitte Access Economics and released in May this year.
It does not reassure.
It’s not news that older people go to the doctor much more often than the young. But it’s perhaps a surprise that the increase starts so early in life. As this chart shows, the number of full-time equivalent GPs needed to treat 25-to-34 year olds is almost three times the number needed by those in their early twenties.

As the population ages, that demand will increase. The average age of GPs is getting older too, so increasing rates of retirement will drive future shortages.
Meanwhile, the amount of work demanded of GPs is increasing rapidly, particularly among women. Despite a slight and temporary downturn in the early pandemic lockdowns, that long-standing trend of increased demand is likely to continue.

Taking into account all the factors they could think of affecting supply and demand, the Access Economics people had a grim prediction. Though the GP shortage in regional and rural Australia was unlikely to improve, it wasn’t going to get much worse either. For people in the cities, it’s a different story.
Most people in the major cities can see a GP when they need to. They may have to wait a bit longer than usual, and it will cost them more. But they’ll be seen.
That situation won’t last. Unless decisive action is taken, city-dwellers will find themselves in a similar situation to those in the bush. In just ten years’ time, the gap between rising demand and falling supply will widen so far that we’ll need an extra 11,500 full-time GPs in the cities just to stay where we are now.

Here’s another way of looking at it. On a percentage basis, by 2032 the cities will need 60% more GPs than they are likely to have.

As we saw earlier, the Medicare rebate for a basic consultation, when adjusted for inflation, is now 44% lower than it was when Medibank began in 1974. Bringing the rebate back to its original value would cost the government just over $4 billion a year. And that’s only for general practice. Raising it by that much across the board would cost $12.6 billion.
That’s not going to happen quickly, and perhaps not at all. The Treasurer, Jim Chalmers, is preparing the nation for a tough budget later this year.
But even if that money was available, would it be enough to fix the problem?
Doctors have now become accustomed to charging their patients, and patients have become accustomed to paying. Under the terms of the Australian constitution, constructing a policy that would ensure a return to bulk-billing would be almost impossible.
But we can start the process. Many practices would welcome the chance of returning to bulk-billing, particularly for their most vulnerable patients. And returning the rebate to its original value would go a long way to decreasing the remuneration gap that currently exists between GPs and other specialists. And so there would be less incentive to charge patients.
If the new Labor government is serious about restoring fairness and access to health care, this money will have to be found. There’s no other way.