
How much longer will dementia be out of control?
The causes are intractable or unknown. Medical research has hit a wall. And we don’t even detect cases effectively.
 |
| Amyloid plaques in Alzheimer's disease |
If dementia was an infectious disease, we’d call it a pandemic. But there’s no vaccine, no effective treatment and prevention efforts are going backwards.
By 2050, according to the official projections, almost half a million Australians will be living with dementia. That’s twice as many as there are now. For people over 85, this cruel disease is now the leading direct cause of death. And it affects almost twice as many women as men.

Several factors are behind this. The most obvious is the ageing of the population: this is almost exclusively a disease of old people.

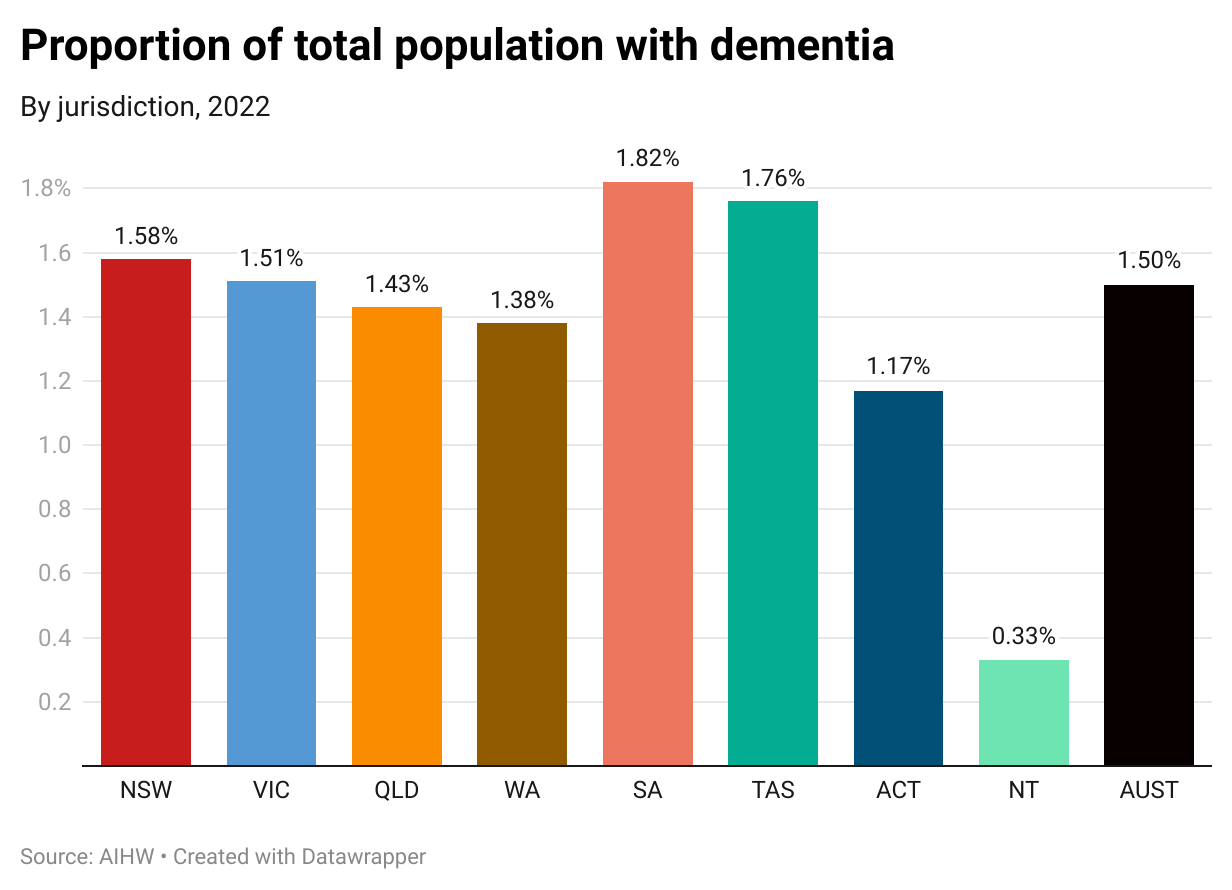
Across Australia, dementia strikes somewhat unevenly. States with generally older populations – South Australia and Tasmania – bear a greater burden. The 2021 census showed that 21% of the Tasmanian population was over 65 and 20% in South Australia. The national average was 17%.
Without major breakthroughs in prevention and treatment, the number of people over 85 living with dementia will rise by 157% – more than two-and-a-half times – compared with today.

Age is the main risk factor. But then there are the usual suspects behind many disorders, including this one: obesity, smoking, high blood pressure, diabetes, lack of exercise, poor diet, high alcohol consumption and low levels of cognitive engagement.
Everything on this list (other than getting older) is, theoretically, controllable. We can take blood pressure medication, lose weight, give up smoking, cut our intake of alcohol and so on. But these factors can be held responsible for only about 40% of all dementia. You have little or no real control over the other 60%, such as genetics, brain injury, gender, and various medical conditions including chronic kidney disease and multiple sclerosis.
And there’s a whole range of other factors, either unproven or still unknown. (And that’s without the furphies – like the social-media flurries that led some people to think that aluminium saucepans cause dementia).
THE BURDEN OF DISEASE
Calculations of the burden of disease measure the total impact of an illness on all the people suffering from it. How many years of life are being lost? What’s the financial cost to the patient and the country? What’s the effect of disease symptoms and treatment side-effects on people’s capacity to live a productive life?
The number of years being shaved off of people’s lives by dementia has been growing rapidly. This measure was 73% higher in 2022 than it was just eleven years earlier.

And we can see who is paying that price: older people, particularly those over 80 and particularly women.

As a cause of death, dementia is now second only to coronary heart disease, which includes heart attacks. And it’s well ahead of the other big fatal diseases, like stroke and lung cancer.

Although dementia is a major killer, someone who develops the condition is still much more likely to die from something else. The two-thirds of patients who eventually die from another condition still suffer harm, ranging from mild to severe.

The mortality statistics, then, only reveal part of the picture. The other part is the impact on people living with dementia. Health economists use a measure called the Disability-Adjusted Life Year, or DALY, a proxy for a year of disability-free life. It takes into account not only premature death but also the overall impacts of living with the illness.
The number of DALYs foregone to dementia rose by 59% in eleven years.

NOT ONLY ALZHEIMER’S
Dementia is a symptom rather than a disease. And there are four main conditions responsible for it:
Alzheimer’s disease is responsible for about two-thirds of all dementia cases but has no scientifically confirmed cause. It is associated with a buildup around brain cells of plaques of the beta-amyloid protein, or fibrous tangles made up of another protein, tau. Despite massive research, drug interventions targeting the development of these plaques and tangles have shown at best only minor clinical benefit.
Vascular dementia is caused by strokes and is believed responsible for about 20% of dementia cases. Vascular dementia can follow a major stroke or a series of minor ones, called transient ischaemic events.
 |
| Robin Williams had Lewy body dementia |
Fronto-temporal dementia is associated with an abnormal buildup of proteins in the frontal and temporal lobes at the front of the brain. These structures have been described as making us human: they control key functions relating to consciousness and communication, memory, attention and personality. It’s less common, accounting for maybe 5% of all cases.
And dementia can be a result of other conditions, including Huntingdon’s disease, AIDS, brain injury, Parkinson’s disease and Creutzfeldt-Jakob disease.
HOW RELIABLE ARE OUR FIGURES? (NOT VERY, ACTUALLY)
Almost all of the statistics I’m quoting are estimates, not certain numbers. Estimates are always wrong – sometimes by a little, sometimes by a lot. Right now, we have no way of knowing. When we try to count actual people, we get results like this:

You’d think that hospitals would have pretty good records of which patients have what disease, particularly as their funding depends on it. But no.
“Unspecified” dementia accounts for 17% of reported cases – an extraordinary number of people for whom either a diagnosis was not made, or made and not reported. The “other” category, at 21%, is equally questionable: according to the Australian Institute of Health and Welfare, this includes several conditions that each account for only a few per cent of cases. And vascular dementia, at 12%, looks massively under-reported.
The AIHW has a project looking at the gaps in essential surveillance. It says this:
“There is no system for monitoring dementia in the Australian community as there is for cancer, diabetes, chronic kidney disease and a number of communicable diseases. According to the [WHO’s] Global Dementia Observatory, few countries operate national dementia surveillance systems.”
We need not only to know which dementia patients have which condition, but also to be able to track those numbers over time. If there are advances in, say, cardiovascular health by controlling obesity, blood pressure and cholesterol, how will we know if that’s reducing the incidence of vascular dementia? At the moment, we won’t. That makes policy decisions much harder and less well-informed than they need to be.
Better access to data, including giving epidemiologists access to anonymised information from various existing databases, is essential. These include access to routine patient monitoring, records of people admitted to hospital, and outpatient records. Of the 17 richest countries, only two – Korea and Sweden – give researchers access to this information. Of the five key information sources, Australia says no to three of them. Belgium, Germany, Ireland, the US and the Netherlands are worse.

CAN WE AVOID THE WORST?
If there is a way out of this mess, it is likely to come in pill form. Pharmaceutical interventions look like the most promising way of dealing with the causes of dementia.
The problem is that we don’t know – at least, not in enough detail – what causes most kinds of dementia. The exception is vascular dementia, which is unequivocally due to stroke – either bleeding onto brain tissue or blockages to blood vessels in the brain.
Researchers and drug companies have long known that Alzheimer’s and most other leading causes are marked by the abnormal buildup of various proteins in various parts of the brain. But drugs targeting those proteins haven’t so far worked very well.
In 2000 I was a member of the Pharmaceutical Benefits Advisory Committee, which decides which drugs should be listed on the PBS, when the first Alzheimer’s drug – donepezil – came onto the market. This drug, marketed by the Pfizer Corporation, binds to and disables cholinesterase, an enzyme which breaks down acetylcholine, an important neurotransmitter chemical.
As this was the first drug for Alzheimer’s, there was a good deal of hype. But much of that initial enthusiasm waned as independent studies questioned just how good the drug was. It was certainly expensive and, according to the normal PBS criteria, nowhere near being cost-effective.
As the committee’s consumer member, I pushed hard for it to be listed and, eventually, prevailed. There was, after all, nothing else that people with Alzheimer’s could look to.
That didn’t make it a particularly effective treatment. It has modest symptomatic benefit in some people with Alzheimer’s disease – probably less than 50%. In dementia related to Parkinson’s disease and in Lewy Body dementia, it slows the progression of the disease in some people but not in others. Some experience significant or serious side-effects. In 2018 the respected Cochrane Collaboration conducted a review of all the available clinical studies and concluded:
“We found that people with Alzheimer's disease who took 10 mg of donepezil a day for six months did slightly better than people taking placebo, on scales measuring their cognitive function (e.g. thinking and remembering), how well they could manage their daily activities, and the overall impression of a trained researcher. We did not find any effect on behaviour or quality of life.”
Since then, two “me-too” drugs in the same class have
appeared on the market: galantamine and rivastigmine. They don’t work any
better. Donepezil, now much cheaper because it’s out of patent, has most of the
market in this drug class. As a lower-priced generic medicine, it's now almost certainly cost-effective for the PBS.
Memantine, a drug in another class, targets the over-production of a neurotransmitter, glutamate, with the idea of modifying some Alzheimer’s symptoms.
All of these drugs modify symptoms but ignore the cause of disease. Three new monoclonal antibodies, aducanumab, lecanemab and donanemab, try to do that by preventing the beta-amyloid protein from forming into dangerous clumps. Aducanumab was approved by the US Food and Drug Administration in 2021 but has proved highly controversial. The FDA approved the drug against the advice of its own expert panel, which found there was insufficient evidence that it slowed cognitive decline and major problems with side-effects, particularly a condition affecting eyesight which can also induce brain bleeds. Three committee members resigned in protest.
The probable failure of this drug (lecanemab and donanemab are not yet approved) casts serious doubt on the main thrust of Alzheimer’s research – the belief that the disease can be successfully treated by counteracting those protein plaques. If that’s not the case, it means a vast amount of global research has hit a dead-end.
 |
| Plaques ... is the core hypothesis wrong? |
Professor Bush is more upbeat about lecanemab. According to the evidence available so far, he says, it’s both safer and more effective. Lecanemab has been approved in the US but Australia’s Therapeutic Goods Administration has yet to receive an application.
Aducanumab is under consideration by a TGA expert committee but its prospects are not good. And it’s expensive: Americans are paying $US56,000 ($A84,000) a year. A US study concluded: “Aducanumab is not cost‐effective at the estimated price of $56,000 even under ideal circumstances in which it completely halts AD progression.”
Even if it’s approved for sale in Australia, it is almost inconceivable that it would be listed on the PBS.
If we can’t treat dementia, can we prevent it?
As we’ve seen earlier in this post, the paths to preventing dementia are largely identical to those for preventing a large range of serious and often fatal illnesses – heart disease, various cancers, respiratory diseases, liver disease and diabetes.
They’re largely about behaviour change – moving people away from dangerous habits to healthy ones. They’re about stopping smoking, controlling weight, avoiding excess alcohol consumption and eating fresh food. They’re also about allowing at-risk people to monitor their health, which has become much more difficult with the decline of Medicare and general practice.
Smoking has been on the way down for many years: only 11% of Australians are still daily smokers and 63% have never smoked. Obesity, a major factor in vascular dementia and of concern in others, is still rising. One of the few bright spots is the introduction of an effective wight-loss medication, semaglutide, in 2019. It works by increasing insulin production (and so diminishing appetite) and decreasing glucagon (boosting energy levels).
It's reasonable to expect newer drugs will be developed that will be more effective and have fewer side-effects. Semaglutide is listed on the PBS for diabetes but not yet for obesity.
So far, other medications protecting cardiovascular health – statins for cholesterol and anti-hypertensives for blood pressure – have not had any apparent effect on population-wide obesity and overweight. In 1995, 4.9% of Australian adults were severely obese; by 2017 that had risen to 11.7%.
This post began by asking how much longer dementia would be out of control and whether the dire predictions of death and disability, with their inevitable impacts on health and aged care services, could be averted.
Something may come along. Let’s hope so, but at the moment there’s little sign of any transformative development. When – if – serious progress is made, it is unlikely to be a silver bullet. Dementia, like cancer, is a massively complex field and, as with cancer, progress is likely to be incremental and agonisingly slow.